A tragic problem caused by crossed wires and a question that still lingers.
CAUSE & CIRCUMSTANCE
When electrical wires are allowed to impinge on aircraft systems and structures, the routine vibrations of flight can gradually abrade the insulation and the wires themselves, resulting in an open path for current to flow where it doesn’t belong. If the adjacent system contains a flammable liquid, such as hydraulic fluid, the electrical energy can ignite the liquid and cause an inflight fire. That’s what happened to a Piper PA-31T Cheyenne in 2016. The investigation raised questions about the effectiveness of maintenance inspections on the accident airplane and other Cheyenne aircraft. An NTSB emergency recommendation and an FAA airworthiness directive on the PA-31T were issued as a result of the accident. However, some observers also believe the methods used to inspect those airplanes represent a “normalized deviation” from the objective measures that were once a standard in aviation maintenance, and they believe those standards need to be restored.
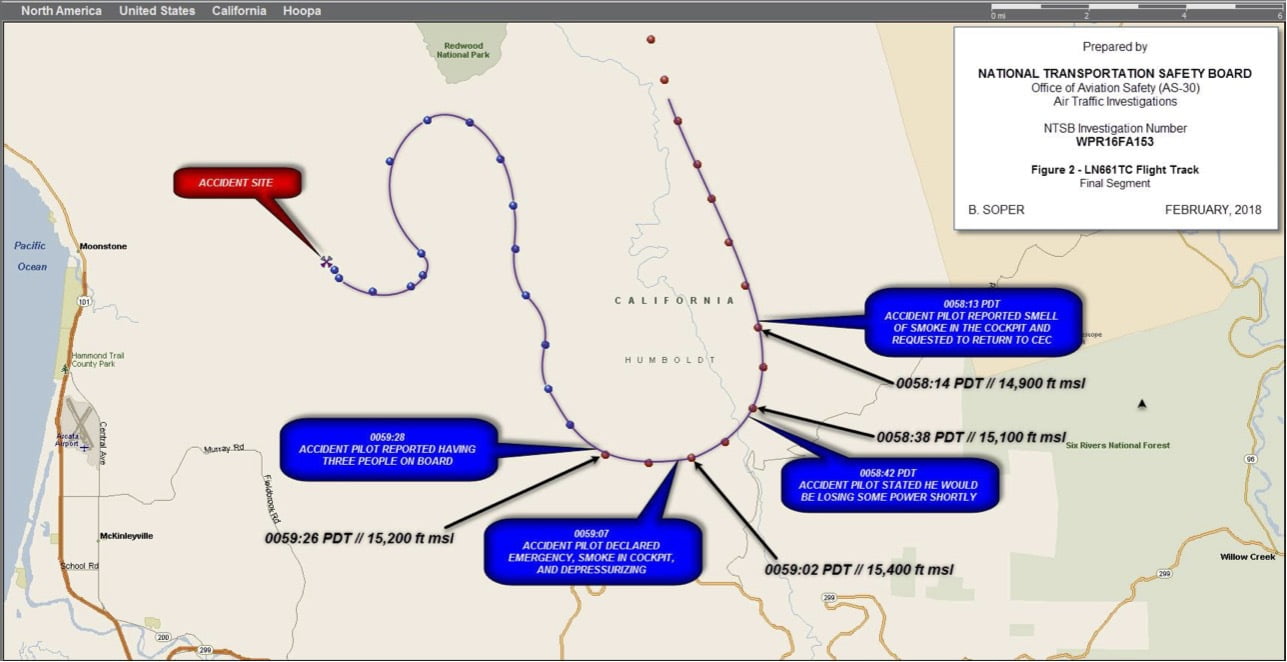
The Part 135 air ambulance, N661TC, departed Crescent City, California (KCEC) at 0045 Pacific Daylight Time (PDT) on July 29, 2016. The flight was operated by Cal-Ore Life Flight on an IFR flight plan, and onboard were the pilot, two medical crew members and one patient. The flight was destined for Oakland International Airport (KOAK), Oakland, California. After takeoff, the flight was radar-identified by Seattle Center and cleared to climb to 15,000 ft. and to KOAK as filed. At 0058, just 13 min. after takeoff and level at their requested cruise altitude, the pilot advised the center they were smelling smoke in the cockpit and they needed to return to KCEC. After being cleared direct to KCEC and down to 9,000 ft., the pilot told the center he may lose power but would try to keep the controller informed. He then declared an emergency and said he would be depressurizing the airplane. He turned right to a northwest heading and asked that the fire department be notified. At 0059:26 the airplane’s mode C radar data dropped off the controller’s radar. The pilot’s last radio transmission was just after that. He said he had three souls on board. Air traffic control (ATC) primary radar returns showed the airplane flew northwest for a little over a minute, then turned southeast. At 0102 it turned west towards Arcata, California (KACV), but at 0102:50 primary radar returns were lost. At that time the airplane was about 6 nm northwest of KACV.
NTSB
A witness located northeast of Arcata reported that in the early morning hours of July 29, she heard an airplane circling overhead and then proceeding westward. After about 15 seconds of silence, and while she was looking out the window of her tent, she saw a large dome-shaped flash to the west, and then another flash and a loud rumble. Skies at the nearby Arcata airport at the time were overcast, and visibility was 1/2 mile. The FAA issued an alert notice at 0210 and a ground search was initiated. Air search efforts were hampered by darkness and fog. The first portions of the wreckage were found at 1011 that morning. There were no survivors. The Investigation Investigators from the National Transportation Safety Board (NTSB), one of whom was a fire expert, arrived at the accident site on the afternoon of July 30. They were accompanied by FAA inspectors, representatives from Cal-Ore Life Flight, a Piper Aircraft air safety investigator, and two County Sheriffs. The wreckage, which was scattered along a 2,400 ft. long path, was located in mountainous, heavily forested terrain just a few miles inland from the Pacific Ocean. One of the first tasks investigators must do at an accident site is establish the location of the four corners of the airplane. In this case, those four corners were not in one place but were scattered along a path oriented about 354 deg. magnetic. The baggage door and part of the horizontal stabilizer were first to land, followed by the vertical tail, the right wing and engine, the left wing and finally the fuselage and left engine. There were numerous fractures in the control system that appeared to be the result of tension overload. Such overload happens when there is an inflight breakup of the airplane. Investigators were not able to establish control continuity.
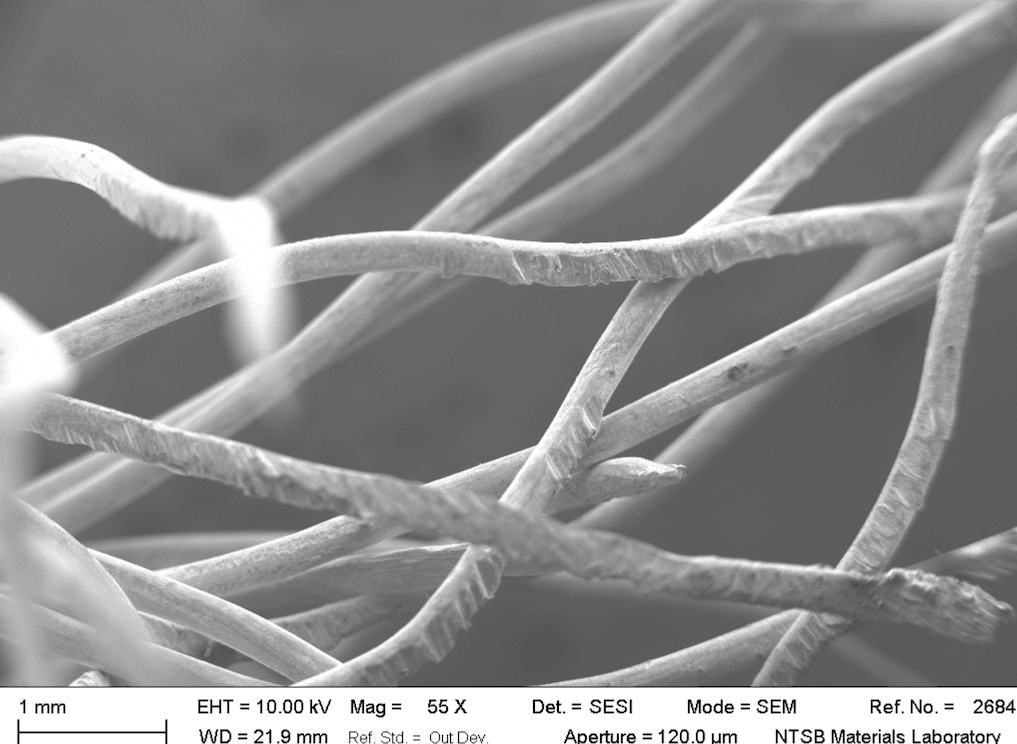
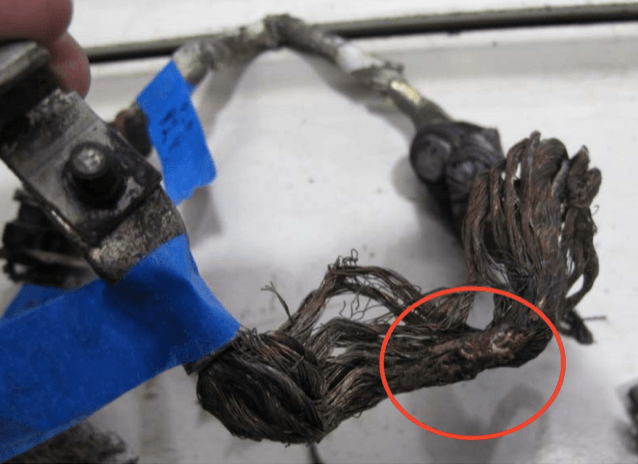
The cockpit and instrument panel sustained extensive impact damage, but other parts of the airplane experienced minimal impact damage. Post-crash fire damaged the inner parts of the wings where the fuel tanks were. The cabin area of the fuselage was intact, but the area between the pilot and copilot seats showed thermal damage. Even though the cabin showed no signs of fire, there was soot coating the exterior skin of the fuselage. The vertical stabilizer, which was 1,260 ft. south of the fuselage, also was covered with soot. The wreckage was moved to a facility in Pleasant Grove, California, for further examination. Investigators found the engines showed no evidence of malfunctions. The fire damage near the pilot seats was primarily in the floor area where the main bus tie circuit breakers were located, although it extended forward to the wing spar. The aluminum structure was melted and torn and the paint was discolored. The circuit breakers were charred and nearby wiring was melted, discolored or missing. Four nearby hydraulic lines showed signs of melting or missing material. The circuit breaker panel, hydraulic lines, fuel crossfeed lines, and high voltage wiring were removed from the airplane and sent to the NTSB’s Materials Laboratory for further examination. A scanning electron micrograph showed notching on conductor surfaces. The aluminum hydraulic lines were heat damaged and fractured. An autopsy performed on the pilot showed that his right boot was melted and the right leg of his flight suit was heat damaged. Both his right hand and right leg suffered burns. The Cheyenne was not equipped with flight data or voice recorders. An Apple iPad and a Samsung Galaxy phone were recovered from the wreckage, but no useful information could be obtained. An air traffic specialist at the NTSB was able to reconstruct the airplane’s flight path using recorded ATC tracking data. The airplane appeared to make a very sharp turn just before it descended into the ground. Without recorded acceleration data, investigators couldn’t say for sure, but to me, this was most likely the point at which the airplane was overloaded and began to shed structural components. The airplane, manufactured in 1981, was powered by two Pratt & Whitney PT6A-135A engines. It had accumulated 7,286.6 flight hrs. and had been maintained on Piper’s progressive 100-hr. inspections. The most recent inspection was just 13 days before the accident. It was equipped with a handheld fire extinguisher and smoke goggles.
The PA-31T has a 28-volt DC electrical system powered by a battery and two starter generators. The main tie bus circuit breaker (CB) panel is mounted in the cockpit floor, with circuits carrying ratings between 50 and 200 amps. Two additional circuit breakers for the Lifeport cabin medical equipment system were in the accident airplane’s CB panel. The 1900-psi hydraulic system operates the landing gear and gear doors, with a separate system for braking.
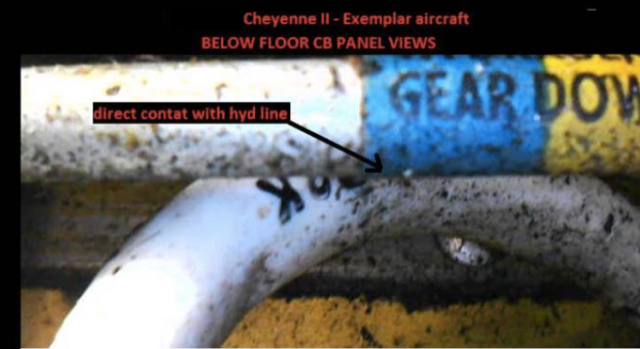
There are four lines carrying hydraulic pressure just under the floor. The airplane’s cabin is pressurized, but the structural bay just below the circuit breaker panel that contains the electrical wires and hydraulic lines is not pressurized. The airline transport-rated pilot had 7,300 total flight hrs. when hired. He had completed his company checkout on the PA-31T on May 12, 2016, and had accumulated 125.5 flight hrs. in the airplane. He was 54 years of age and had a class II medical certificate that required he have available glasses for near vision. On the two nights before the accident, he had flown a total of 5 hrs. 45 min. Cal-Ore Life Flight is an on-demand Part 135 operator based in Crescent City, California. At the time of the accident, the company operated 7 PA-31T aircraft and employed 12 pilots. The FAA’s Part 135 aircraft registry shows the company operates five King Air’s and an R-44 helicopter, but no Cheyennes. Looking at Other Cheyennes Sixteen months before the Cal-Ore crash, another Cheyenne had crashed just short of the runway at Fort Lauderdale Executive Airport (KFXE) shortly after the pilot had reported smoke in the cockpit. He exclaimed “mayday, mayday” five times before the airplane pitched over into a wooded area about 1/4 mile from the runway and burned. On autopsy, that pilot’s blood was found to have 4% carbon monoxide and he had some soot in his upper airway. His three passengers, who were the pilot’s wife and two daughters, had elevated carbon monoxide in their blood, with levels of 17%, 20% and 72%, respectively. Their upper airways contained soot. The pilot died of blunt force trauma, but the passengers died of smoke and fire injuries. The airplane’s last inspection, an annual inspection, was accomplished just nine days before the accident. Despite an extensive investigation, the NTSB could not determine the source of the fire. The center fuselage and cockpit were consumed by fire. The Board’s probable cause was “a rapid onset of smoke and/or fire inflight for reasons that could not be determined due to the post-impact fire and the condition of the wreckage.” Seeing a possible connection between the two accidents, investigators decided to look beyond the Cal-Ore crash for a more systemic explanation for the fires in the Cheyenne. They first examined two PA-31T’s in Cal-Ore’s fleet. Using a small high definition video camera and a borescope passed through an electrical lead access panel in the fuselage, they found electrical wires passing in close proximity to hydraulic lines. On the first airplane, one wire passed less than 1/2 inch from a hydraulic line and another was in direct contact with a hydraulic line. On the second airplane, the right generator circuit breaker wire was in direct contact with one of the hydraulic lines. FAA inspectors found several additional PA-31T aircraft to examine. Between the NTSB and the FAA, a total of six exemplar airplanes were examined, and on each one, electrical lines and hydraulic lines were found in direct contact. In some cases, they also found chafing between hydraulic lines and electrical wires.
Conclusions and Actions Before the National Safety Transportation Board (NTSB) had completed its report, the FAA issued Special Airworthiness Information Bulletin (SAIB) CE-17-05 on Dec. 16, 2016. The bulletin, which was not mandatory, alerted owners and operators of five PA-31 models to inspect and repair chafed, burned or damaged wires; repair loose or corroded terminals; re-route wires as needed; and notify the FAA of any findings. It also cited an excerpt from AC 43.13B, one of the FAA’s primary guides to inspections, that says wiring and fluid lines must be positively clamped so as to be no more than 0.5-in. apart. The guidance in the SAIB was described as a “best practice,” not a requirement. On Jan. 5, 2017, the Board issued its report. The NTSB determined the probable cause of the accident to be “an inflight fire in the floor area near the main bus tie circuit breaker panel that resulted from chafing between an electrical wire and a hydraulic line and/or airplane structure.” The Board also issued safety recommendation A-17-001 to the FAA, which stated, “Issue an emergency airworthiness directive (AD) that requires owners and operators of Piper PA-31T-series airplanes to take the actions recommended in Special Airworthiness Information Bulletin CE-17-05 immediately after the AD is issued. Urgent.” Multiple actions then took place in fairly rapid-fire order. On Jan. 6, Piper Aircraft issued service bulletin (SB) 1301, which directed inspections and repairs to the CB panel. Boxed in red letters was the statement “Piper Considers Compliance Mandatory.” The instructions in the SB included the statement “Reroute or rework as necessary to minimize the likelihood of chafing contact between adjacent components such as fluid carrying lines, airframe structure, and other wiring.” The FAA issued airworthiness directive (AD) 2017-02-06, effective on February 22, which mandated the previously recommended inspections and repairs in the Piper service bulletin, and further required repetitive inspections at least every 12 months. On April 27, 2017, the NTSB closed their recommendation A-17-001, saying the actions taken were acceptable. So, the problem was solved, or so it seemed. How Should Inspections Be Done? Two lingering questions remain. Why did two airplanes catch fire and crash so soon after being inspected? And, if six nominally airworthy airplanes were found with unacceptable contact between wires and fluid lines, how many supposedly safe airplanes are out there in similar states, waiting to catch another pilot and his passengers unawares? One answer could be the criteria used to do inspections. This is the point made by Pete Kelley, a 21-year FAA airworthiness inspector, in an article called “Methods, Techniques, and Practices--the Lost Requirement for Criteria.” Writing in the July-September 2021 issue of the ISASI Forum, a magazine for air safety investigators, Kelley says the determination of whether a given condition is airworthy should not depend on who is making the determination. There should be objective criteria. The FAA’s AD 2017-02-06 just follows the subjective language of the Piper Bulletin. The 0.5-in. clearance in the SAIB was dropped, and “minimize the likelihood” inserted. “Minimize the likelihood” is not an objective criteria!. The guidance leaves the standard for what is acceptable to the judgment of the technician who does the work, along with the person doing the inspection. Even though the NTSB recommended the FAA carry out the objective standards that are “best practices” in the SAIB, the actual airworthiness directive, the document with the force of law, only directed the use of subjective standards. It would be interesting to know why. As pilots, we count on the mechanics with inspection authorization (IA) to check all work done on our airplanes and ensure it’s done right. I wonder if the FAA’s AD would have been more effective if objective standards were required. In organizations where there is pressure to get the work done and out the door, there will always be the temptation to say “good enough” and let a problem go unaddressed if the criteria for the repair is not clear. When the NTSB closed its recommendation, they seemed to close the door on this potentially important safety issue. I think it will have to be addressed in a future investigation.
—A former military, corporate and airline pilot, Roger Cox was also a senior investigator at the NTSB. He writes about aviation safety issues.