Analyzing the Challenger flight that stalled on short final at Truckee.
IMAGINE WHAT WOULD HAPPEN IF AUTOMOBILES HAD TWO STEERING wheels, two instrument displays and two sets of pedals on the floor. There would be bent fenders, jumped curbs and even some high-speed rollovers when the two people in the front seats differed about which way they should go and how fast. Airplanes, which evolved with such dual controls, survive because pilots are trained and conditioned from their first flight to follow a basic rule: Only one pilot can control the airplane at a time.
Two pilots flying a Bombardier Challenger broke that rule during a critical phase of flight, while lining up with the runway on short final. The result was an aerodynamic stall and a catastrophic crash, with the loss of everyone on board. Why two experienced pilots would make such a basic mistake is hard to explain. The National Transportation Safety Board (NTSB) said poor crew resource management (CRM) contributed to the cause, but there were other risk factors at work, as well.
Credit: NTSB
The Bombardier Challenger 605, N605TR, departed Coeur d'Alene Airport-Pappy Boyington Field (COE), Coeur d’Alene, Idaho, at about 11:45 PDT on July 26, 2021. On board were the two pilots and four passengers. Their destination was Truckee-Tahoe Airport (TRK), Truckee, California. The airplane was newly acquired by charter operator Aeolus Air Charter, but was being operated under Part 91 as a personal flight.
The two pilots had never met one another before they commenced the flight. The pilot designated as pilot in command (PIC) had been offered a position as a charter captain for Aeolus, but was flying under contract rather than as an employee. He had flown one contract trip for Aeolus that terminated in COE. The second-in-command (SIC) was an experienced contract pilot being paid a flat rate to fly the trip. He had commuted into COE from another assignment on the East Coast.
Both pilots had sound credentials. The 43-year-old captain had an Airline Transport Pilot (ATP) certificate issued by Mexico, and type ratings in the CL-600, CL-604, G-200 and LR-60. He had 5,685 total flight hours—3,080 of which were as PIC, and 235 of which were in the Challenger. His most recent flying job, a 4-month contract in the Middle East, ended in February 2021, and he logged only 12.3 hr. in the 90 days before the accident. After he completed a video interview over Zoom with company officials, he attended training at FlightSafety in Wilmington, Delaware. He completed his last proficiency check in the CL-605 on July 16, 10 days before the accident.
The aircraft, N605TR. Credit: NTSB
The aircraft in a fireball after the crash. Credit: NTSB
The co-pilot, who was 58 years old, had 14,401 flight hours. He had 12,355 hr. as PIC and about 4,500 hr. in the Challenger. He had an ATP and six type ratings, including the CL-604 and CL-65, and he had been manager of flight standards, check airman and aircrew designated examiner for PSA Airlines. He was a flight instructor and was also glider-qualified. He said he preferred flying as a contract pilot to full-time employment, and had been active, logging 37.9 hr. in the last 90 days. A review of his recent flights showed that he switched back and forth between PIC and SIC, depending on the needs of the client. He had also recently attended recurrent training at Wilmington, completing his last proficiency check on June 18, 2021.
The flight began routinely, with the captain flying the airplane and the co-pilot reading checklists and handling the radios. The co-pilot spoke deferentially to the captain, but in keeping with his experience as an instructor and check airman, he began prompting the captain about checklists and the planned profile of the flight. A close review of the cockpit voice recorder (CVR) transcript reveals the tone in the cockpit gradually changing. The relationship between the two pilots, sometimes referred to as command gradient, became inverted, with the co-pilot taking the initiative more and more.
During climbout, the co-pilot asked the captain what runway he planned to use at Truckee, and the captain said Runway 11. After leveling off at FL370, the captain left the cockpit to check on the passengers. When he returned, he began a lengthy formal briefing for the approach at TRK, but was interrupted by the co-pilot, who asked, “So you do want to do the approach, or do you want to stay visual?” The captain replied that he wanted to fly the area navigation (RNAV) approach.
Then, as the captain continued his briefing, the co-pilot asked: “Did you ... did you already program that?” The captain said, “I have ... no, I have not programmed nothing.”
In the ensuing conversation, it was evident the captain was not very familiar with this airplane’s flight management system (FMS). He said: “In which book can I see ... where the ... where ... is all the equipment that this aircraft has ... I mean ... uhh ... L-P-V L-D L-NAV P-B-N G-N-S blah blah blah ... where can I see it?”
The co-pilot loaded the RNAV approach and explained details of the system. They also discussed the fact that basic information about the airplane’s weight and balance had not been loaded.
Salt Lake City Center cleared them direct to TRK. When the captain started to proceed direct to the Mustang VOR, the co-pilot reminded him they were not cleared there, but to the airport.
Resuming their discussion about weight and balance, the captain said, “OK ... what's that meaning of LEMAC?” As the co-pilot began to explain the basics of arm and moment, the captain said, “Why don't they put those kind of notes?” and “I have (aircraft) work to do with you.”
The sound of the TRK automated weather observing system (AWOS) was recorded: “Airport automated weather observation one niner five one zulu weather wind zero eight zero at five, visibility seven clear below one two thousand, temperature three two Celsius dewpoint five altimeter three zero one four, remarks density altitude eight thousand niner hundred ... Truckee traffic be advised actual visibility may be different than what is shown on AWOS due to heavy smoke.”
As the airplane commenced its descent, the co-pilot asked, “Are you going to be on the headphones or are you just going to whisper,” and then said “okay it’s ... one or the other ... (but/’cause) I can’t hear you whispering.”
Apparently the captain had not listened to the AWOS, because he asked the co-pilot to recite the airport conditions. The co-pilot provided the information, but overlooked the note about smoke. His workload was going up, and it was about to get worse.
APPROACH CHANGESTruckee Airport, at 5,904 ft. above sea level, sits in a bowl. Mountains just to the south and west rise to more than 9,000 ft., and Mt. Rose, at 10,785 ft., lies just to the east of the airport. The airport authority warns pilots about potentially difficult conditions on its website. Under the heading “Pilot Essentials,” it tells pilots to expect mechanical turbulence, gusty winds and a diverse fleet of aircraft, including jets, light airplanes, flight instruction and gliders operating at the airport. The airport is in a non-radar environment, and no precision approaches are available. Density altitudes often exceed 9,000 ft. in summer. Notably, the site says, “Wildfire smoke can dramatically decrease visibility.”
RNAV (GPS) runway 20 at Coeur d'Alene Airport-Pappy Boyington Field (COE), Coeur d’Alene, Idaho. Credit: FAA and NTSB
July, the month of the accident, is also the busiest, as the two pilots were about to find out.
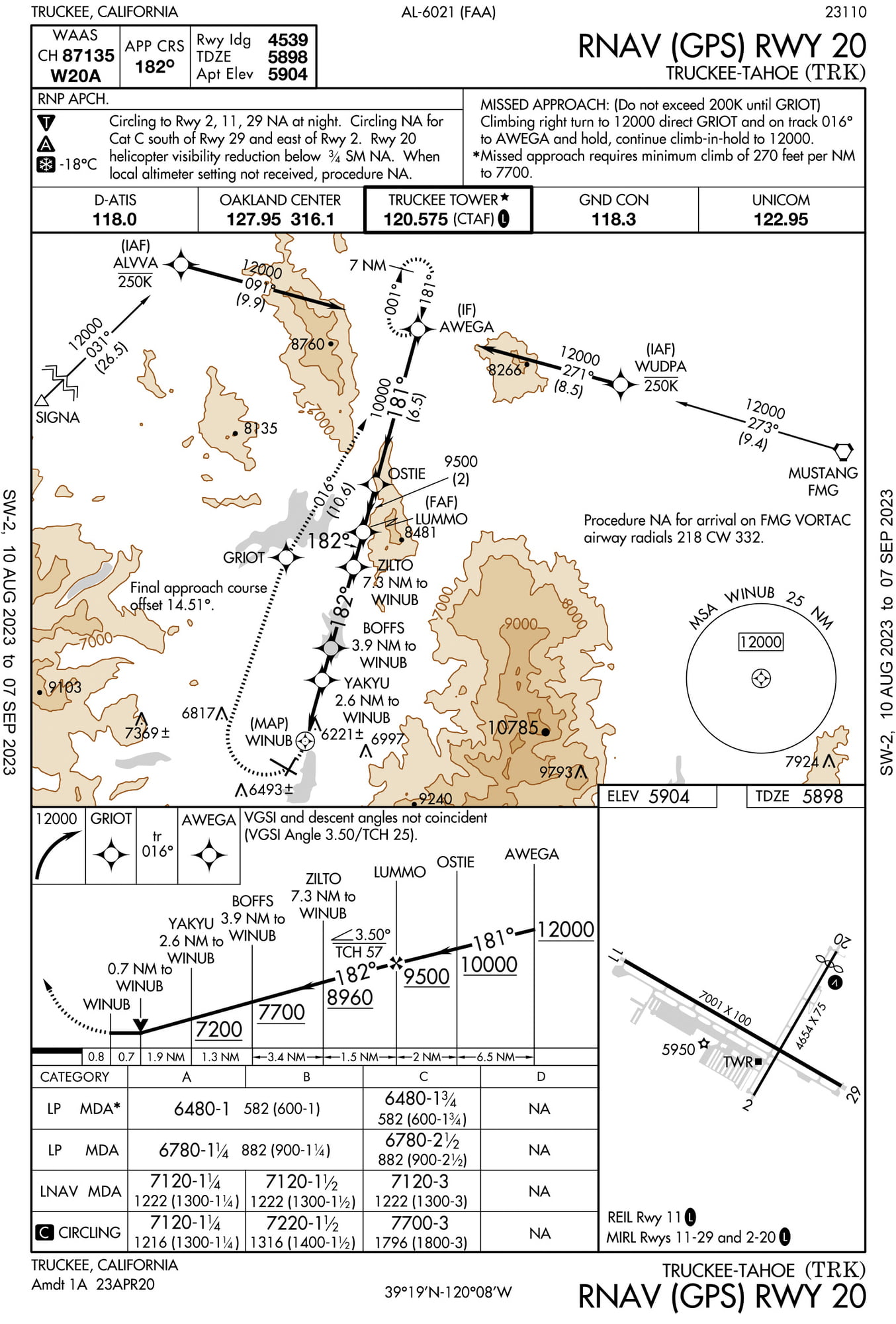
When descending to FL 200 and cleared to ALANT, an initial approach fix (IAF) for the Runway 11 approach, Oakland Center called and changed the approach. It would now be the RNAV to Runway 20, and they were cleared to a different fix, AWEGA. The captain promptly said that runway was too short. He said, “For Runway 20 ... so we will have to circle to land ... so we can't ... cannot accept that.”
They did accept that. They would have to circle to the longer runway, maneuvering at low altitude in unfamiliar, mountainous terrain. They were also number three for the approach and would have to enter holding. Oakland then gave them another change: Holding would not be at AWEGA, but at ALVVA. They were already passing AWEGA when they got the holding clearance.
Since that fix was west of the fix toward which they were already proceeding, they needed to make a sharp right turn. The co-pilot said “I'm gonna start the turn for ya 'cause we're missing it.” The captain said “thank you,” and “I don’t know what it is.”
The co-pilot quickly entered the holding instruction in the FMS, showed it to the captain and told him he could now build the new approach. Events were moving fast. As they were trying to get oriented to the holding pattern, Oakland said “november five tango romeo descend and maintain one four thousand expect the approach shortly.”
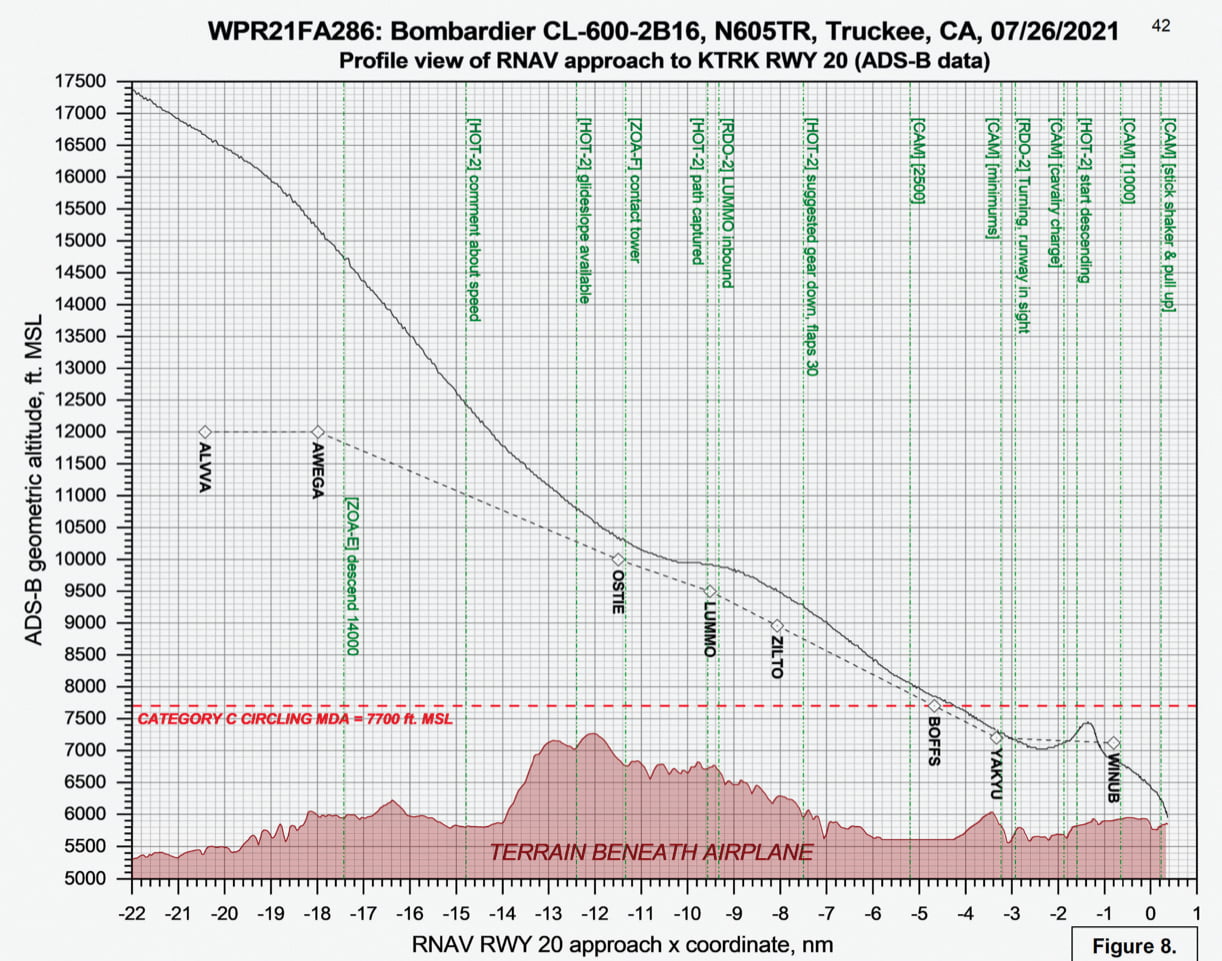
When they were cleared for the RNAV Runway 20 approach, they were at 21,225 ft. above mean sea level. They were going back to AWEGA to start the approach and needed to be at 12,000 ft. when they crossed that fix. The co-pilot asked, “Are you gonna be able to get down?” The captain replied in the affirmative. From that point on, they struggled to get down and remained above the approach charted profile until reaching YAKYU, only 3.4 nm from the airport.
Their speed was also high. Past the IAF, calibrated airspeed was still 250 kt., and ground speed was 300 kt. The co-pilot said, “Gotta get this thing slowed down.” He suggested they do a 360-deg. turn to lose altitude, but the captain declined, saying “No, I can do it.” They started deploying flaps and gradually began to slow.
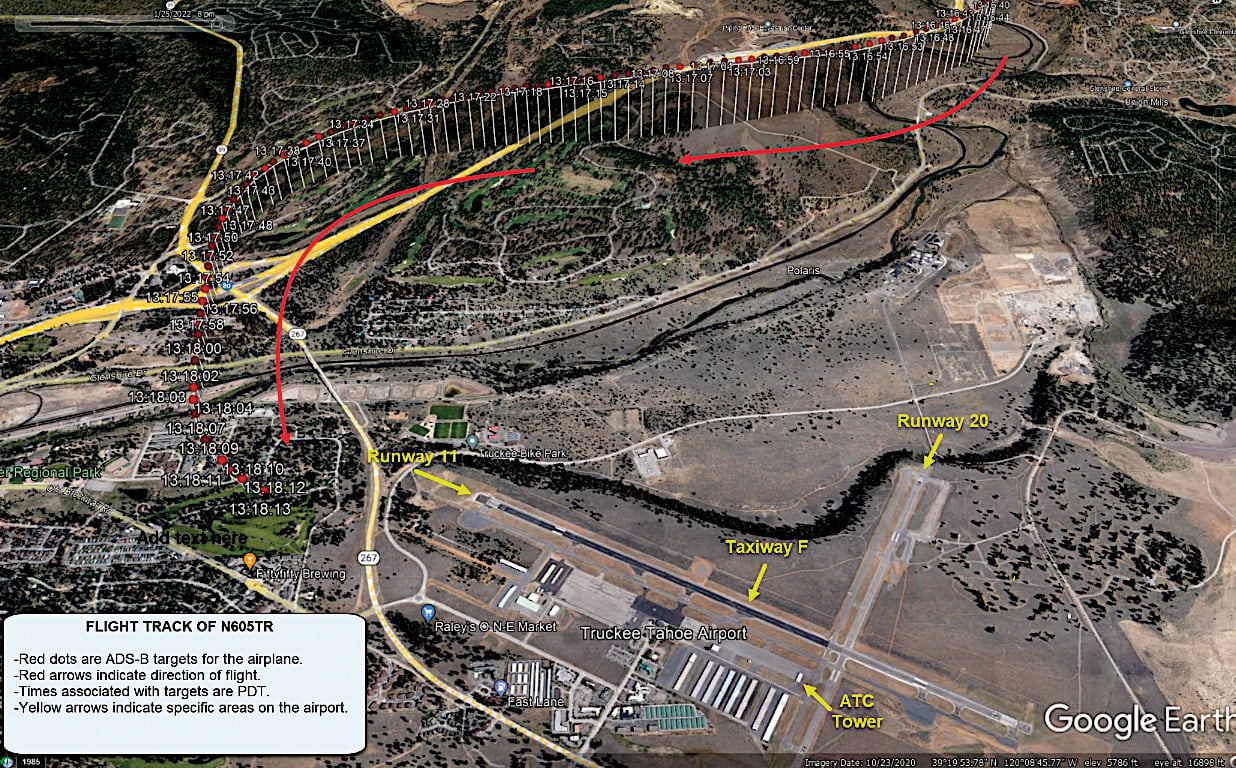
When the co-pilot checked in with Truckee Tower, the tower said, “Challenger six zero five tango romeo Truckee tower uh ... roger report the airport in sight when you're breaking off the approach you can either enter the downwind for one one or you can enter ... you can enter a uh left downwind for one one or you can go over the top left downwind for two nine.”
TRK suggested runway 29 arrival. Credit: Truckee Airport
The traffic pattern depiction on the Truckee Airport website shows overflying the airport and entering a left base for Runway 29 is recommended. The two pilots had apparently not checked the website. They were still looking for the airport.
While the co-pilot was finishing the radio call, the captain called “gear down,” and the co-pilot said, “oh [expletive] you came off ... what are you ... ah never mind.” His composure was starting to fray. He said he had intermittent ground contact, then while he was trying to run the before-landing checklist the captain said, “So it’s to the left, right?” The co-pilot told him, “It’s to the left.”
As the electronic voice announced “approaching minimums,” neither pilot could see the airport. Then, even though he was in the right seat, the co-pilot saw it and realized they were in too close. He said, “Make a right-hand turn 90 deg.” The tower cleared them to land, but the captain just asked “Where?”
They were well within the 3-nm circling radius for their category C airplane, but the captain did not set up a downwind. Instead, he took up a heading that angled toward the final approach course. Seeing both the runway and the developing overshoot, the co-pilot called out, “Roll out ... turn the autopilot off,” and “I’m going to get your speed under control for you.” The airspeed was 162 kt., well above the maximum for circling of 140 kt. The power came back, the airplane began to slow, and the captain finally picked up the runway. However, they were high and overshooting the runway centerline.
The co-pilot began asking to take control of the airplane, a request he repeated four times. The spoilers deployed to their full open position. A sink rate warning sounded, followed by a stick shaker and a pull up warning. The captain cried out, “What are you doing?” as the co-pilot continued to ask for control of the airplane. The stick pusher engaged, and the airplane entered a rapid left roll. The nose fell through, and the airplane descended rapidly into the ground. A large fireball erupted.
Investigators from the NTSB were assisted by representatives from the FAA, Bombardier, TSB of Canada, Rockwell Collins, Midwest ATC Service and General Electric. Both the flight data recorder (FDR) and voice recorder were recovered, and the quality of the recordings was excellent. The recorders showed that there were no airplane systems or engine malfunctions. The investigation focused on operational factors and aircraft performance. Top officials at Aeolus and simulator instructors who trained the pilots were interviewed, and a performance specialist analyzed the airplane’s flight path and flight controls to determine what caused the airplane to stall.
N605TR’s profile of descent. Credit NTSB
Airworthiness investigators discovered that the basic operating weight (BOW) entered into the airplane’s FMS was wrong. It had defaulted to a standard weight of 24,000 lb. because a maintenance provider had not uploaded the actual BOW. The actual BOW was 26,244 lb. As a result, the FMS computed a Vref landing speed of 118 kt, which is 6 kt slower than the proper Vref of 124 kt.
The performance study showed the discrepancy did not contribute to the stall because the airplane was flying faster than the correct reference speed before it stalled. The study showed that it was the full deployment of the spoilers about 12 sec. before the accident than most degraded the stall margin.
A review of the pilots’ certifications and training showed they were qualified to conduct the Part 91 flight. But analysis of their performance on the accident flight found three significant failures.
■ They flew the circling approach at a speed exceeding the limit for their category C approach category.
■ They failed to establish a proper downwind leg of the circle-to-land maneuver.
■ They failed to see the runway early in the approach, probably because visibility was reduced by smoke.
The crew should have abandoned the approach when it became unstabilized. The co-pilot apparently got on the controls even though the captain never relinquished them. Both pilots forgot about safety as they attempted to salvage the approach. They lacked clear communication and failed to recognize their own degraded performance and vigilance.
HIRING, TRAINING AND CRMThere were two parts to the NTSB’s probable cause: the co-pilot’s steep turn, and the captain’s failure to correct the co-pilot’s actions. There were three contributing factors: the co-pilot’s deploying the spoilers, the captain’s poor setup of the circling approach and both pilots’ self-induced pressure to perform and poor crew resource management (CRM).
While these conclusions are certainly true enough, looking at the facts with a different lens produces some additional issues. If, in addition to the crew’s unsafe acts and environmental factors, we look at supervisory and organizational factors, there is more to the story.
The company, Aeolus, took a very hands-off approach to the accident flight. They put pilots they barely knew into the cockpit of a newly acquired airplane they themselves had not properly inspected. The youthful entrepreneur who was the CEO had ambitions to grow and then sell the company, but he lacked aviation knowledge and experience commensurate with his responsibilities. He hired the accident captain without checking his visa status and did not realize he was not eligible to be a full-time employee. Had he checked, the captain would not have been piloting on the flight.
None of the company’s managers questioned whether the captain, who had been idle for a while, might need more training and familiarization than he received at the Part 142 school and by reading the company’s general operations manual online. None of the managers looked into the risks of flying into Truckee, which was affected by forest fires and was a tricky place to fly into—especially on one of the pilot’s first flights in the airplane. The managers seemed to rely heavily on the internet and Zoom to find and screen applicants. Interviews with the managers revealed a kind of cut-and-paste hiring mentality, matching credentials with needs instead of in-depth personnel decision-making.
There were far more risks to the accident flight than seemed apparent at the beginning. If either pilot had done some homework and checked the Truckee Airport website, they could have planned accordingly. The website is very candid about the potential hazards there. The airport says many accidents occur during attempted circling approaches. The NTSB database lists 79 accidents at TRK—more than Aspen, with 33, and even more than JFK, with 73.
Even the most diabolical simulator instructor could not have constructed a more difficult scenario than what the two accident pilots encountered. They had multiple revised clearances with no notice or time to adjust. They experienced true airspeeds about 20 kt. greater than calibrated, and that probably contributed to the overshoot. They were surprised by how much the smoke from all the forest fires reduced the visibility and hampered the captain’s awareness of the airport layout. He may have refrained from turning all the way to downwind for fear of losing sight of the runway.
The captain was behind the airplane almost from the start of the flight. It seemed like he did not know where he was most of the time. The co-pilot, in contrast, knew exactly where he was and what to do. He got more and more frustrated as the flight progressed and the captain resisted his help. He was so confident in his ability to maneuver the airplane that he tried to salvage an increasingly untenable approach. As we see so often, the increasing stress of a developing bad situation caused tunneling of attention in both pilots.
Hardest to accept are the actions of the co-pilot. Patient, alert, knowledgeable and experienced, he let his guard down at the last minute. As a contract pilot, and before that as a check airman, he switched back and forth between left and right seats constantly. As the SIC, calling for a go-around would have been appropriate; grabbing the controls was not. Adjusting from instructor to PIC to SIC blurs the roles and makes it hard to stay in character. Ironically, he knew this. He had accepted a job as an FAA inspector in order to quit contract flying and have a more regular schedule with a clearer role.
—A former military, corporate and airline pilot, Roger Cox was also a senior investigator at the NTSB. He writes about aviation safety issues.