A faulty localizer and descending below decision altitude caused this crash.
When it comes to flight and navigation instruments, there are few absolute certainties. Even though most instruments are fairly reliable, they are all susceptible to error. Altimeters can be high or low, airspeed indicators inoperative, attitude and heading indicators can roll over or spin down. Pilots learn to look for the signs of these failures.
One of the instruments pilots have learned to trust is the instrument landing system (ILS). If the frequency is tuned and identified, there are no warning flags, and the flight director pitch and roll steering bars are centered, you can feel pretty confident that you are on centerline and on glidepath, in a position to land right in the center of the runway. A regional jet crew attempting to land in Presque Isle, Maine, found out that even the trusty old ILS can sometimes lead you astray. On March 4, 2019, CommutAir Flight 4933, an Embraer EMB-145XR, struck the snow-covered infield to the right of Runway 1 at Presque Isle Airport (KPQI) while attempting to land. On that wintry day, the visibility for landing was at the very minimum allowable for that approach, 0.5 mile, and there was moderate snow and freezing fog. The airport was also uncontrolled, so there was no tower to issue last-minute information or to coordinate airport snow-clearing activities. The flight crew followed their localizer indication perfectly and wound up in the grass, 305 ft. to the right of the runway centerline. An entire chain of safety barriers had to fail for the accident to happen. Before the crew made their last mistake, many other people had dropped the ball. The story shows how even minor oversights by people in safety supporting roles can be significant. The flight originated in Newark, New Jersey, a major hub for CommutAir’s major partner, United Airlines. There were two pilots, one flight attendant and 28 passengers aboard, and the estimated time en route was 1:39. At 1003 EST, the flight took off, and shortly thereafter they climbed to FL350. At 1049, they commenced a descent and began to prepare for the approach. The weather was concerning. The 1056 automated METAR was wind, 080 at 6 kt.; 0.5-sm visibility; snow; freezing fog; 1300 overcast; temperature, -2; dew point, -4; altimeter, 29.70. At 1055, Boston Center read them the KPQI FICON (field condition) NOTAM for Runway 1. “You have ah field condition of three, three, three, one hundred percent, quarter inch dry snow, and ah yup that should be it, there is also a quarter inch dry snow on ah all of the taxiways as well braking action reported as medium, and ah half inch of dry snow on the apron.” At 1059, the first officer (FO) briefed the ILS approach to Runway 1, saying ”There are no lights just the MALSRs down there, expecting what about a half mile and eleven hundred feet down there it shouldn't be that bad if we do have a missed approach it'll be a TOGA check max thrust flaps nine positive rate gear up, ahm we'll do it with the box ah let's climb to a hundred ah eleven hundred left turn to three thousand direct to PQI VOR and hold.” The two pilots agreed to make a second approach if they missed on the first one. (Runway 1 was equipped with high-intensity runway lights.) At the FO’s command the captain read the descent and approach checklists, and the FO replied that they were complete. The captain tuned and identified the KPQI ILS, then selected the NAV approach button. Boston Center cleared them for the approach and at 1103, the captain called “Go green now—zero zero six,” then “forty-one thirty-one.” After prompting, the FO called for flaps nine and said the “LOC’s captured.” At 1105, Boston Center said “CommutAir forty-nine thirty-three radar services terminated, change to advisory frequency approved, cancel on the ground one two one point six or with me in the air ah twenty-four seventy-five.” The captain canceled IFR and switched to the KPQI CTAF. When the airport’s maintenance manager replied, she told him she was 4 min. out. The runway was clear. The glideslope came alive, the crew extended the landing gear and flaps to 20, set speed bugs and set the altitude alerter for the missed approach altitude of 3,000 ft. They then went to flaps 45, completed the landing checklist and the captain called out passing the final approach fix. She said, “Thousand to go, stable,” and “ground contact.”
The left main landing gear was lodged between the left engine nacelle and the fuselage. Credit: NTSB
When the captain clicked the mike switch five times, the FO reminded her the airport lights frequency was 122.6, and she then repeated the five clicks. The captain made callouts at 500, 400 and 300 ft., and the FO then said, “Autopilot comin’ off.” An electronic voice called “autopilot, autopilot,” then “approaching minimums.” Following her 100-ft. call, the captain said, “Runway in sight. See it?” The FO replied, “Yeah—well I got somethin' looks like a runway up there.” Actually, there was nothing there. The crew had made a textbook approach up to this point, and then they made their first error. They were lined up, not with the runway, but with an AWOS antenna well to the right of the runway. As the FO looked out, he allowed the nose to rise, prompting the captain to call out “Watch your speed yeah watch watch your, go, go up, go up, go up, go up, go up!” The stick shaker sounded. Again, she called, “Go, go missed, go missed.” “TOGA, check thrust flaps nine.” “Go, go, go,” she exclaimed. The FO apologized for “looking at the wrong thing,” but when the “don’t sink” voice came on the captain said again, “Go up, go up, go up!” The “landing gear” master warning sounded. The captain handled the warning, made the missed approach radio call, and got the gear and flaps up. She got the airplane settled down and turned around and began preparing for a second approach. The crew seemed baffled about what went wrong. The FO asked, “What the heck happened?” The captain said, “I thought I had the runway then it was like that is not the runway!” After the captain’s brief reply, the FO then asked, “Did you ever see the lights at all last time?” Her reply was equivocal. “It’s really white down there—that’s the problem.” The crew’s strategy for the second approach was essentially the same as for the first except for one thing. The FO planned to focus hard on the ILS flight director steering bars, even below 200 ft., and wait for the captain to positively identify the runway. The captain said, “Just stay on the flight director and the glideslope and ah a lot of times what I’ll do is I’ll stay in there ’cause otherwise once you go out visually ah, you know, you start going high and low and then it gets really screwed up.” The FO replied, “That’s just me being a rookie…. I just realized my error last time—I was overconfident. After I went visual, I quickly realized that was the wrong way to do business.” The captain said, “Yeah, stay inside and I’ll let you know when you can look up.” This strategy, based on a misperception of what happened, was also contrary to company policy. The policy stated the pilot flying should monitor the instruments until the callout “runway in sight,” then transition to outside references no later than 100 ft. Thirteen minutes after the missed approach, Boston Center again cleared CommutAir 4933 for the ILS to Runway 1. The FO immediately said, “Got the ground already this time.” At 200 ft., the FO disconnected the autopilot at the captain’s direction. When the electronic voice announced, “minimums, minimums” the captain said, “Alright runway in sight twelve o'clock lights are ah.” “OK I'm stayin' on the flight director 'cause I don't see it yet.” Ten seconds later the first sounds of the hard landing were recorded. Again, the captain said, “What the ####” and the FO said, “I don't know what I'm seein’.’’ The pilots still did not know what they had done. Eleven seconds later, someone is recorded on the cockpit area microphone. “I got it, I got it, the localizer was ####.” Finally, the pilots understood what happened. The crew ran the engine shutdown checklist and began to coordinate with the flight attendant to conduct an evacuation. According to the flight attendant, the landing was rough and violent. She had all the passengers remain seated until the L1 door was open. Firefighters walked through deep snow to reach the airplane, then a snowplow cleared a path to the door. A ladder was raised to allow the passengers to deplane. A firefighter helped the FO, who had a head wound, to exit first. Snow around the airplane was up to the bottom of the fuselage. Besides the FO, two passengers sustained minor injuries. The Investigation The NTSB conducted what is commonly known as a “field major” investigation, later categorized as a limited (Class 3) investigation. It was assisted by the FAA, CommutAir and the Air Line Pilots Association. The investigation took three years and four months to conclude and no recommendations were issued. The airplane came to rest 3,600 ft. beyond the approach threshold, 305 ft. to the right of the runway centerline, and 230 ft. to the right of the right runway edge. An airworthiness group visited the accident site the day after the accident and spent three days documenting the wreckage. Much of the airplane was intact. There was obvious damage to the nose, which was damaged back to the first bulkhead on top and back to the nose gear position on the bottom. The nose gear wheels were located aft of their normal position; there were scuffs, dents and scratches on the wing leading edges; and there were broken flap jackscrews. There were cracks and shifts in flap panels. The airplane’s localizer antenna appeared to be undamaged. The left main landing gear was lodged between the left engine nacelle and the fuselage, and the right engine inlet was damaged. There was minor interior cabin damage, the most notable of which was two small holes in the fuselage wall near seat 24A. In addition to the two crash recorders, ADS-B data was available from the FAA. A performance specialist and an ATC specialist used that data to reconstruct the flight path. An air traffic control group met with staff from Boston Center to discuss what happened from ATC’s point of view. They learned that a crew had reported the localizer discrepancy to the center after landing at KPQI on March 2, two days before the accident. During an approach to Runway 1 the pilot noticed a significant localizer offset to the right. His call to the center was recorded. He said there was a “good offset the right of the localizer there all the way down—ah—became visual about ah two thousand five hundred or so and ah once we were center with the runway the localizer was about half dot off all the way to the ground.” The controller acknowledged the report and said he would pass it on. The ATC group interviewed the FAA National Airspace Systems operations manager. He had received the message but declined to follow up because FAA procedure is to confirm any report of a navaid malfunction with a second report before taking action. There were no flights into KPQI after the one that reported the discrepancy. The FAA conducted a post-accident flight inspection of the KPQI ILS on March 7 and found that the localizer was indeed out of tolerance by 200 ft. to the right. They also found a glideslope anomaly. After snow was cleared from around and in front of the localizer and glideslope antennas, the ILS was retested on March 13 and the signals were within normal tolerances.
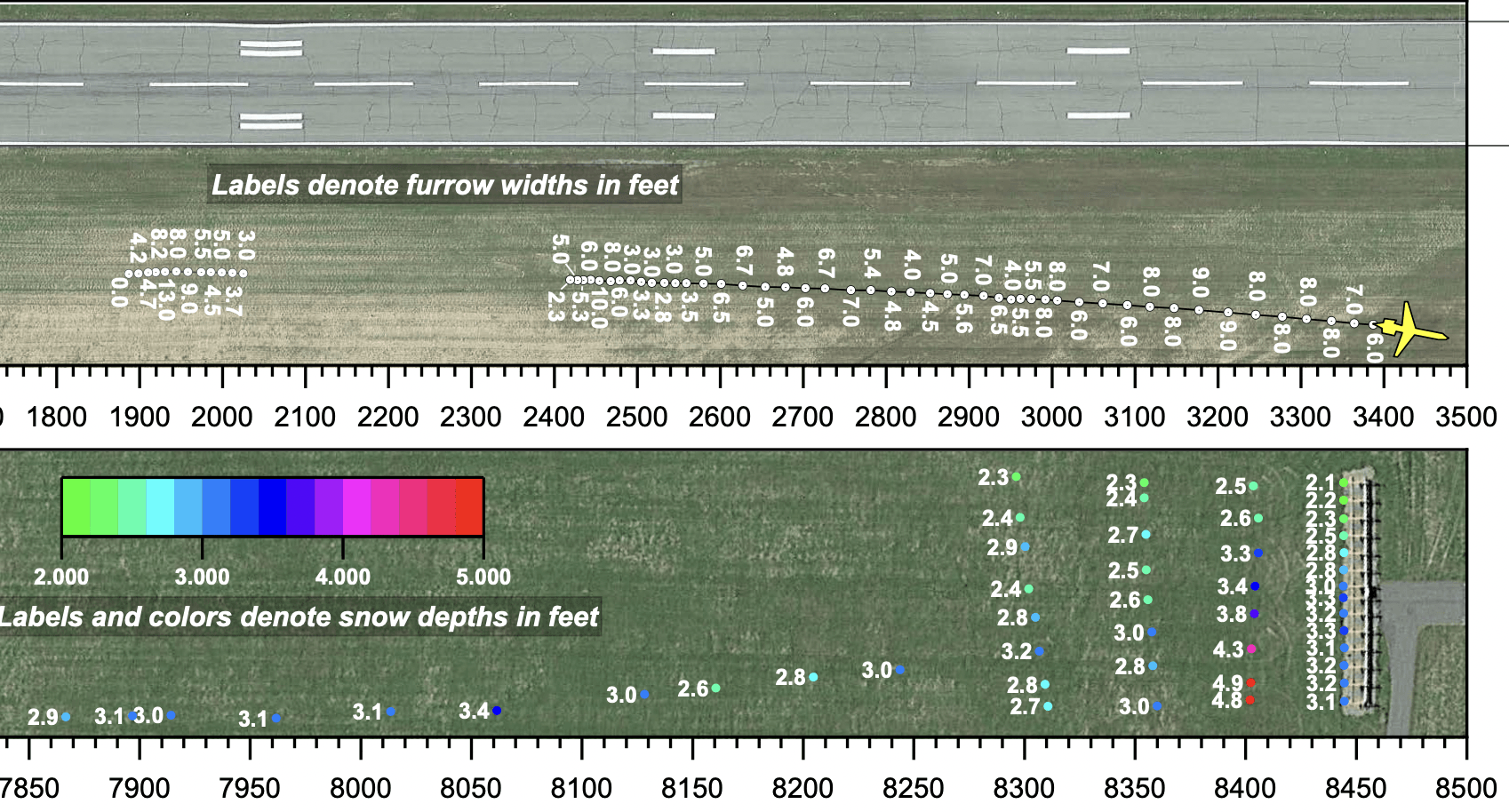
Snow depths in feet at Presque Isle, Maine. Credit: NTSB
An NTSB airport specialist investigated events that took place at KPQI before, during and after the accident. He obtained airport surveillance videos that showed the airplane going around and later enveloped in a snow cloud during the landing. He learned that the lightning arrestor atop the wind sensor pole of the AWOS installation was bent. The only reasonable conclusion was that it was struck by the airplane, although the NTSB declined to say so. KPQI maintenance staff scraped off the snow around the antennas using bulldozers and a tractor. It took over 15 hr. Before beginning to plow, they measured snow depths in front of the localizer antenna. There were four berms or ridges in front of the antenna that rose as high as 4.9 ft. Airport operations staff reported that there had been localizer signal problems in previous years, and they had been resolved by FAA technical personnel. Typically, when a signal was out of compliance, they removed snow. However, they never knew exactly how much to remove. The FAA’s Advisory Circular on Field Conditions (AC 150/5200-30D) specified snow clearance values for glideslope antennas, but not localizer antennas. Eight months after the accident, the FAA modified the AC to set 2 ft. as the limit of snow before a localizer antenna must be evaluated. An Operational Factors/Human Factors group investigated the pilots and CommutAir’s management, policies and procedures. The 40-year-old captain had a somewhat checkered career. She had accumulated 5,655 total hours and 1,044 hr. on the EMB-145 but had moved around between airlines in the midst of proficiency issues. She left her first job at Republic Airlines after failing to pass her ATP check, then joined CommutAir as an FO. She had a stint at Virgin America, where she completed a type rating in the Airbus A320 but returned to CommutAir, again as an FO. The company delayed her upgrade to captain, and when she attempted to upgrade on the EMB-145 she was disapproved for steep turns and engine failure takeoff. She completed her upgrade in October 2017 but remained on an “increased scrutiny” status with the company. Check airmen were very complimentary about her performances on a LOFT (line-oriented flight training) and proficiency check in 2018. She had no accidents or incidents before the accident in KPQI. The 51-year-old FO had accumulated 4,909 total hours of flight time and 470 hr. in the EMB-145. His experience was mostly in FAR Part 91 operations before he was hired at CommutAir in May 2018. He completed his EMB-145 type rating in July of that year with no noted difficulties. His most-recent recurrent training was two months before the accident. The NTSB found two physiological concerns for him: a recent bout of flu just before the accident flight, and not using his CPAP (continuous positive airway pressure) machine. The night before the accident flight he had less than normal sleep, and probably was in a 2- to 3-hr. sleep deficit. CommutAir had an FAA-accepted safety management system program in place, and it included FOQA and several safety reporting systems. One safety manager said the company received over 700 ASAP reports a year but had received no pilot reports about the KPQI localizer. Six CommutAir pilots had noted the localizer discrepancy at KPQI in the five days before the accident, but none had reported it to the company. The accident FO was one of these pilots. Conclusions and Comments In thinking about all the ways this accident could have been avoided, the first thing that comes to mind is the captain calling the runway in sight when she did not have a view of the landing surface at all. The second thing is the FO should have gone no lower than 100 ft. because he never saw a runway either. Both broke the fundamental rules listed in 14 CFR Part 121.651 about when you can descend below the decision altitude to touchdown. The NTSB explained the pilots’ actions as the result of confirmation bias. They explain that “Confirmation bias is an unconscious cognitive bias that involves a tendency to seek information to support a belief instead of information that is contrary to that belief.” The perfectly crossed ILS steering bars were certainly a strong reason to believe the flight was in the right place. This situation could have fooled many pilots. The NTSB came out with a safety alert in 2011 about avoiding “rote callouts.” Several accidents had taken place after pilots had called out indications that hadn’t happened. “Thrust reverse deployed,” “spoilers deployed,” “lift dump,” “flaps.” These were part of repetitious, highly proceduralized routines done in a short time span. The pilots were so used to making the standard callouts, they missed actually verifying the indication they expected to see. Judging by the cockpit voice recorder transcript, the captain was a wizard at standardized procedure. It seems to me she made the “runway in sight” callout more from rote memory than real visual contact. The NTSB also faulted the FO’s fatigue state and the failure of pilots to report the localizer anomaly. The NTSB’s probable cause was “The flight crew’s decision, due to confirmation bias, to continue the descent below the decision altitude when the runway had not been positively identified. Contributing to the accident were (1) the first officer’s fatigue, which exacerbated his confirmation bias, and (2) the failure of CommutAir pilots who had observed the localizer misalignment to report it to the company and air traffic before the accident.” I question the wisdom of having the FO fly the first leg of a trip when the two pilots haven’t flown together before. It’s an important time to establish roles, captain’s authority and personal preferences. Some companies also require the captain to fly approaches to low minimums. One tip-off for this captain’s decision was her remark about “going up and down” when transitioning to visual conditions. She wouldn’t believe that if she were herself proficient in low-visibility landings. There’s one more factor to consider here. A whole slew of people could have prevented this accident if they had been more safety conscious and more proactive. The ATC manager could have closed off the ILS until someone had time to check its signal. The KPQI operations staff could have asked for an FAA ILS check when the snow got so deep. The airline’s certificate management office (CMO) could have been more alert to winter hazards at KPQI. The pilots who noticed the problem could have reported it immediately. And last of all, the accident FO could have put two and two together and been ready for the localizer signal to be off-center, having already noticed it on an earlier flight. Aviation must have a culture of continuous vigilance, not just by pilots, but by everybody. Safety is not someone else’s job.
—A former military, corporate and airline pilot, Roger Cox was also a senior investigator at the NTSB. He writes about aviation safety issues.